The concept of Quality by Design (QbD) was implemented by the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) and United States Food and Drug Administration (FDA) around a decade ago, with the aim of adopting systematic approaches for developing high-quality pharmaceutical products for patients’ benefit and to meet regulatory needs…
QbD does not just facilitate product and process understanding, it also increases regulatory flexibility, enabling faster approval of products with reduced numbers of recalls and rejects. With the ascent of time, a series of guidances have been published by ICH and endorsed by the FDA for harmonising the holistic implementation of QbD paradigms in pharmaceutical manufacturing. This has certainly revolutionised traditional testing-intensive pharmaceutical manufacturing.
This webinar showcases the Growth Direct System; an RMM (Rapid Microbial Method) that improves on traditional membrane filtration, delivering increased accuracy, a faster time to result, enhanced data integrity compliance, and more control over the manufacturing process.
Key learning points:
Understand the benefits of full workflow microbiology quality control testing automation in radiopharmaceutical production
Learn about ITM’s implementation journey and considerations when evaluating the technology
Find out how the advanced optics and microcolony detection capabilities of Growth Direct® technology impact time to result (TTR).
Don’t miss your chance to learn from experts in the industry –Register for FREE
Can’t attend live? No worries – register to receive the recording post-event.
QbD has brought enormous benefits to the development of drug substances, analytical methods, dissolution testing, stability studies, bioequivalence testing and clinical trials. Regulatory agencies are encouraging the pharmaceutical industry to holistically implement QbD in all of these stages to reduce product development times, and accelerate regulatory review and approval processes. This article endeavours to provide an overview on vital precepts of QbD paradigms during different stages of development for efficient pharmaceutical manufacturing to produce a robust product with the desired safety and efficacy.
Introduction
For decades the pharmaceutical industry has been continuously engaged in developing new drug products and generics to cater for healthcare demands and serve the patient community. However, owing to the involvement of active drug substance(s), multiple functional/nonfunctional excipients and manufacturing processes that lack automation, pharmaceutical products are facing a high degree of variability in their quality, which has become a major topic of debate.
In 2002 a news article published in The Wall Street Journal stated:
“although the pharmaceutical industry has little secret…, yet its manufacturing standards lag far behind potato chips and laundry soap makers”,
while another article published in 2007 mentioned that the:
“pharmaceutical industry is producing six-sigma products using three-sigma processes”1,2.
These news articles shook the entire pharma world, but demonstrate that assuring consistency in the quality of drug products is a major point of concern, and something that is taken seriously by the federal regulatory agencies.
To revolutionise quality standards, regulatory agencies started focusing on the pharmaceutical manufacturing standards and approval process. In 2003 the FDA proposed the first major quality initiative in the form of “Pharmaceutical cGMPS for the 21st Century-A Risk-Based Approach” to safeguard patients’ health with the promise of delivering high-quality drug products3. This demonstrates that systematic science- and risk-based approaches were starting to be adopted during product development practices. Later, the International Conference on Harmonization (ICH) instituted a series of guidances including Q8 (Pharmaceutical development), Q9 (Quality Risk Management) and Q10 (Pharmaceutical Quality System) for harmonising the adoption of quality principles by industry and regulatory agencies4-6. All three guidances are interrelated, although Q8 primarily focuses on precepts and fundamental elements of QbD.
The concept of quality is not new to the world and has been important in manufacturing practice since the 1980s. Motorola was the first company to implement the use of systematic quality principles into manufacturing practice, which later percolated into several technology-driven industries including information technology, telecommunication, automobile and aeronautic7. However, such principles were adopted in pharmaceutical development much later. After the institution of ICH Q8-Q10 guidances, the FDA started coercing the pharma industries to adopt QbD paradigms to improve their manufacturing standards.
Figure 1: Quality triology as per the Juran’s quality philosophy.
Based on the principles of six-sigma, the QbD concept was first outlined by an American quality expert, Joseph M. Juran, through his publications and book, “Juran on Quality by Design”8. He described the concept in the form of Juran’s triology, where quality is considered as a dynamic trait and undergoes continuous improvement by the act of conscious intent with apt planning and control. Figure 1 illustrates the concept of Juran’s quality triology, which aims to deliver products with the goal of quality by planning but not by chance9. Moreover, Juran also enunciated the philosophy of building quality into the products by design to avoid the traditional practice of quality by testing.
Quality Planning
This involves planning the quality at the very first stage based on the “voice of customer”
Quality Control
The variability in product and process attributes needs to be controlled by adopting risk-based statistical tools for monitoring the end-product quality
Quality Improvement
This is a continuous process, which is achieved throughout the product life cycle by regulating the controls
Pharmaceutical QbD: Fundamental principles
Based on Juran’s concept, pharmaceutical QbD primarily takes the approach of envisioning and planning product quality based on predefined objectives. It increases product quality and robustness; increases customer satisfaction; reduces defects, recalls and rejects, thus ultimately providing significant savings of resources such as time, effort and cost. Beyond these, there are several long-term benefits of QbD10,11. Below provides a detailed account on the benefits of QbD:
Reduces development time
Minimises product cost by multiple times
Helps in effective troubleshooting
Facilitates timely launch of the products
Increases consumer generic acceptance
Monitors regulatory oversight with greater flexibility
Maintains product life cycle with greater ease
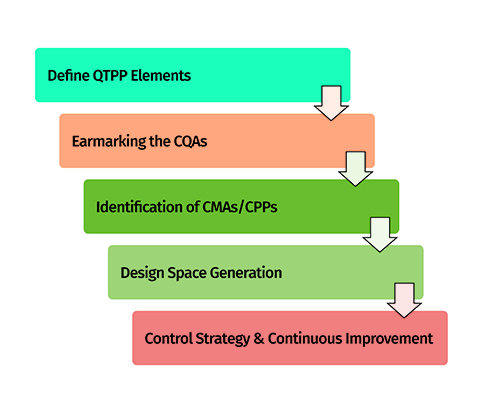
The implementation of QbD in an industrial scenario can be achieved through five key steps, which are discussed in the following sections12,13. These steps work alongside the principles of six sigma, in order to develop high-quality robust drug products with enhanced product and process understanding. Figure 2 portrays the key five steps of QbD on which the product development process is based. These steps are highly important and mandatory in the form of minimal requirements for regulatory approval of drug products.
Figure 2: Five-steps approach for implementation of QbD.
Step 1: Defining the objectives and quality planning
Systematic planning among product development team members is essential for identifying product development objectives before development begins. As per the QbD approach, it is referred to as a quality target product profile (QTPP), which summarises the quality characteristics of the target product. QTPP primarily includes vital product features such as dosage form type, dose, route of administration, pharmacokinetics and stability, which need to be strictly monitored throughout the product development exercise14.
Step 2: Identification of product quality attributes
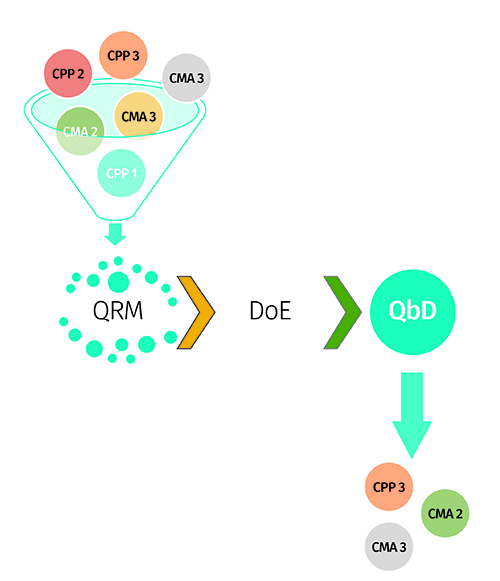
After defining QTPP, the key quality attributes directly associated with product quality are considered while identifying the key vital critical quality attributes (CQAs). The CQAs are also referred to as potential indictors of the product quality performance and directly related to QTPP11,13. These are identified after concerted team efforts to suitably justify their need with respect to their importance in benefitting patients. Instances of CQAs include physical, chemical, biological and microbiological attributes of the drug product, which need to be critically monitored with respect to their defined specifications to avoid inconsistency in the product quality4. As per the QbD-based approach, the desired goals for CQAs are achieved using DoE and QRM principles to identify the critical material attributes (CMAs) or critical process parameters (CPPs), followed by optimisation of them using multivariate experimental designs (Figure 3).
Figure 3: Amalgamation of QRM and DoE approach for factor screening and optimisation.
Step 3: Establishment of specifications on target quality
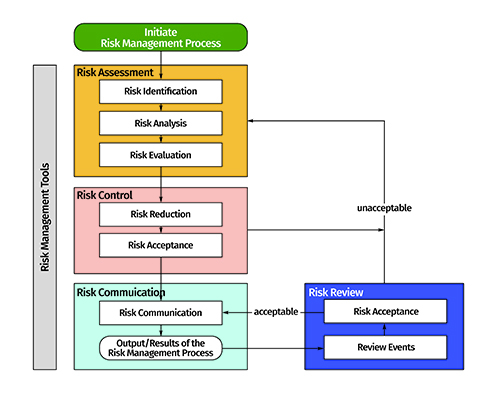
The approach of establishing set specifications for the target product’s quality is carried out by identifying a suitable design space. It is a multidimensional region generated between the CMAs or CPPs, which have direct influence on the product CQAs. Risk assessment or factor screening studies are primarily used for identifying the “vital few” CMAs/CPPs from the plausible “so many”10. Figure 4 depicts the critical steps involved during risk assessment and risk mitigation exercises in an industrial set-up. Risk estimation matrix and failure mode effect analysis techniques are primarily used for risk assessment, while screening experimental designs, such as Taguchi, Plackett-Burman and fractional factorial designs, are used for factor screening purposes12.
Figure 4: Risk identification, risk assessment and risk mitigation as per the QRM approach (adapted from ICH Q9 guidance: www.ich.org).
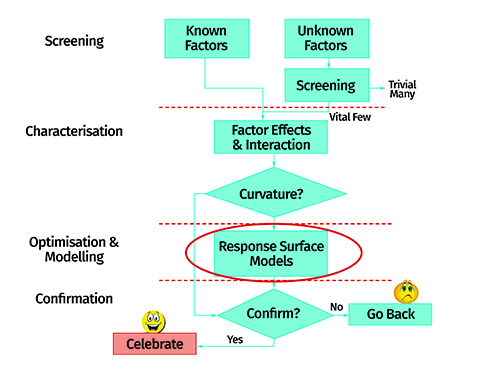
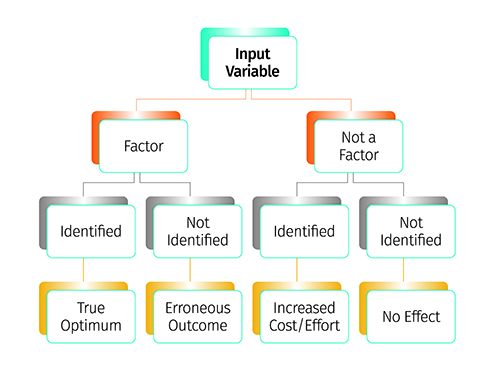
Figure 5 shows a pictorial flow chart depicting the importance of the factor screening exercise during QbD-based product development and optimisation. Moreover, response surface designs such as full factorial, central composite, Box-Behnken, optimal and mixture designs are used for optimisation of the CMAs/CPPs.
Figure 6: Schematic flow layout of the response surface optimisation method.
Figure 6 portrays the steps encountered during response surface optimisation-based product development. The major goal of such optimisation is to identify the design space. The design space is demarcated within the defined specification limits for the CQAs.
Figure 5: Factor screening study depicting the identification of influential factors.
Following submission of the product development report, the design space is approved by the regulatory agencies – thus it is also termed a “proven acceptable range (PAR)”. Movement within the approved specifications of the design space is allowed without any prior notification(s) to the regulatory agencies, while movement outside the design space is considered as “change” and requires further regulatory approval.
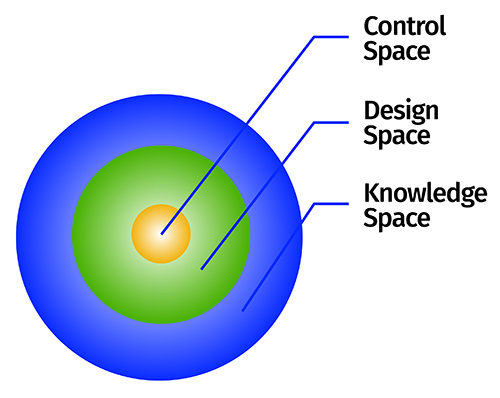
Regulatory agencies are encouraging the industry to identify a control space (also called “normal operating range”) within the design space, on the basis of in-house specifications, to work in a narrower and more constrained region13. Figure 7 pictorially demonstrates the layout of different spaces and their regulatory importance during product development and approval processes. Various types of design space tend to exist during product development cycles, which include lab scale, pilot scale and commercial scale design spaces. Among these, only commercial scale design space has real-time importance for regulatory review and approval of the products14.
Figure 7: Depiction of various spaces as per the QbD concept.
Step 4: Validation of quality specifications
Evaluation of the robustness of design space is carried out by performing ‘edge of failure’ studies. Since design space established only at commercial scale has regulatory importance for product approval, validation of lab scale design space at pilot, exhibit and commercial scale is considered to be essential. As per the federal demands, the sponsor should demonstrate the robustness of design space at commercial scale followed by product and process understanding14.
Step 5: Quality control strategy and continuous improvement
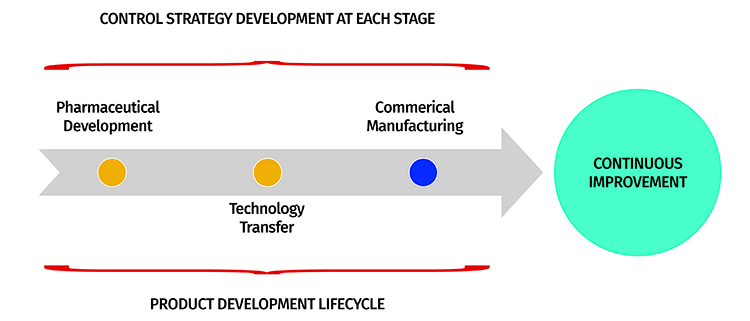
Based on the entire product development exercise, the firm must establish a control strategy for enabling continuous improvement. These include different types of controls used to ensure the product’s quality, including in-process and end-product testing13. It helps with monitoring the product performance at key stages of a product’s life cycle, including development, technology transfer and commercial manufacturing. Figure 8 illustrates a control strategy during these stages of a product development lifecycle. Postulation of control strategy at these vital stages tends to facilitate change management and reduces its impact on the product’s quality to avoid a quality crisis.
Figure 8: Control strategy flow layout at different product development stages.
Pharma QbD: A lifecycle approach
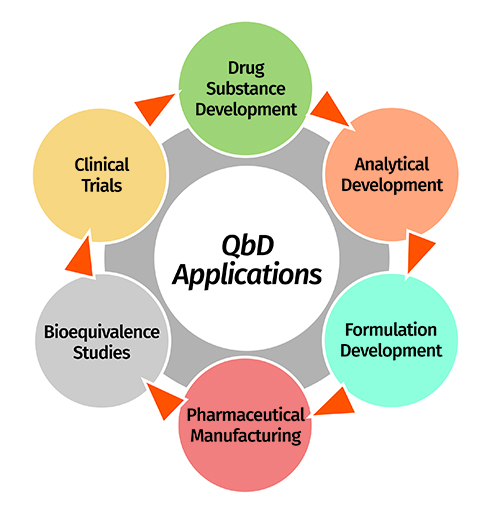
Besides formulation development, the QbD concept has now permeated into other vital areas of pharmaceutical development including drug substance development, analytical method development, dissolution testing, stability testing, bioequivalence testing, clinical trials, etc.15. It is therefore considered to be omnipresent during each of these vital stages of product development. A formulation scientist can even continue to derive QbD benefits after a product’s commercial launch and post-marketing surveillance. A brief account on QbD implementation at various product development stages is given as follows (also pictorially depicted in Figure 9.
Figure 9: Potential applications of QbD approach in diverse stages of product development lifecycle.
Drug substance and excipient development
The quality of finished products depends on the use of high quality raw materials, which includes drug substance and excipients16,17. Variability in these raw materials produces end-products with highly variable quality, and so implementing QbD principles helps to improve the quality of raw materials supplied by the vendors to pharmaceutical manufacturers. The key CMAs of drug substance include particle size, physical form, polymorphism, moisture content and flow properties, which impact the disintegration, dissolution, compaction and compression characteristics as the CQAs. Likewise, the key CMAs of excipients include particle size, shape, viscosity grade, moisture content, flowability, etc., which also significantly influence the aforementioned CQAs. Moreover, the specifications enlisted in ICH Q11 guidance are applicable to QbD requirements for drug substance development along with critical measures on chemistry, manufacturing and control processes18.
Analytical method development
Use of a robust analytical method is essential for hassle-free monitoring of quality and accelerating the product development process. QbD principles, in this regard, facilitate the development of highly robust analytical methods based on predefined objectives or quality target method profile. Critical method variables (CMVs) are identified on the basis of critical analytical attributes for attaining enhanced method performance for continuous improvement within the design space19. In a nutshell, QbD provides a framework to identify the source of variability and reduce it during analytical method development, thus going beyond the traditional ICH recommended validation process20. Although analytical QbD is not mandatory and no regulatory guidelines yet exist, the federal agencies are encouraging the pharmaceutical industry to adopt the implementation of systematic QbD paradigms for improving analytical understanding.
Dissolution testing
Considered as a quality control tool, dissolution testing helps to monitor the drug release profile of dosage forms. This helps the manufacturer to make decisions in qualifying the batches on the basis of release criteria. In this regard, establishment of a discriminating, robust and predictable dissolution method is imperative. A QbD approach provides greater flexibility during dissolution development by optimising the influence of multiple factors, such as media type, composition, volume, apparatus selection and operating conditions on drug release performance. Regulatory agencies today demand highly robust drug products with an in vitro dissolution performance close to that of the reference listed product, so establishing a predictable in vitro/in vivo correlation for the accomplishing biowaiver21.
Stability testing
Implementing QbD principles in stability testing helps to establish specifications (temperature and humidity conditions, packaging materials, etc.) for stability testing of the products and monitoring controls for identifying the product shelf-life, levels of impurities, degradation products, etc.22. As the concept gains importance in product development, the number of long-term regulatory benefits will rise.
Bioequivalence testing
Bioequivalence tests are used for the final assessment of the in vivo product performance and to evaluate the plausibility of matching between the generic product and reference product24. Vital pharmacokinetic metrics such as the Cmax and AUC ratio between the test and reference products must be within the regulatory acceptance limit of 80%-125% for bioequivalence. In this regard, QbD furnishes formulation development by establishing a link between the input product and process parameters to optimise the in vivo performance. The concept has limited regulatory importance owing to the lack of practical understanding in establishing direct correlation between the in vitro and in vivo product performance parameters.
Clinical trials
The application of QbD principles to clinical trials is one of the most recently investigated scenarios. Such an approach examines the design and objectives of a clinical trial protocol by identifying the ‘critical to quality’ factors and managing the impact of risk on trial quality. Since high expenditures are incurred from clinical trials, federal agencies have been emphasising the current opportunities with QbD risk-based monitoring of clinical studies to help bring about the best possible scientific outcomes for product safety and efficacy.
Conclusion
QbD applications that can address multiple challenges and quality issues are increasingly being used at different stages of pharmaceutical product development. An organisation can reap maximal benefits of QbD by collaborating closely with internal departments to work synergistically for holistic product development practices. Regulatory agencies are also encouraging drugs manufacturers to adopt a greater number of science-based approaches that improve the quality of products and provide benefits during question-based review processes.
Declaration: The views expressed herein are the views and opinions of the authors and do not reflect or represent the views of any of the organisations with which the authors are affiliated.
Biographies
SARWAR BEG, PhD is a Research Scientist at Jubilant Generics Limited, Noida, India. His major areas of research interest include QbD-driven development and characterisation of diverse drug delivery systems. To date he has authored more than 90 research/review publications in several peer-reviewed journals, 15 book chapters, four books, three Indian patent applications with h-index of 16 and several young scientist awards to his credit. Moreover, he is serving as the Regional Editor of Current Nanomedicine, Editorial Board Member of Bioavailability and Bioequivalence Journal and Nanotech Research Letter, and reviewer of several international journals.
MAHFOOZUR RAHMAN is an Assistant Professor at the Department of Pharmaceutical Sciences, Faculty of Health Sciences, Sam Higginbottom Institute of Agriculture, Technology & Sciences (SHIATS), Allahabad, India. He completed his Masters in Pharmacy in 2010 from Jamia Hamdard, New Delhi, India. His major areas of research interest include development and characterisation of nano-size drug delivery systems for inflammatory disorders. To date he has published over 50 publications in peer reviewed journals with H-index of 12 and eight book chapters with various reputed publishers. He is a member of IPGA and editorial board member of various journals.
MR SAGAR SUMAN PANDA is currently working as an Assistant Professor at Roland Institute of Pharmaceutical Sciences, Berhampur, Odisha, India. Mr Panda has seven years of teaching experience in pharmaceutical analysis and major research interest in QbD-based analytical method development and validation. He has over 35 research publications in various peer-reviewed journals, one book on analytical QbD and several conference presentations to his credit.
References
New prescription for drug makers: Update the plants. The Wall Street Journal. 2002: CCXLII
Making improvement work in pharmaceutical manufacturing. ISPE Midwest Extended Education and Vendor Day, Overland Park, KS. 2007
Pharmaceutical cGMPS for the 21st century — A risk-based approach. 2004
ICH Harmonised Tripartite Guideline. Q8(R2)-Pharmaceutical Development. 2004
ICH Harmonised Tripartite Guideline. Q9-Quality Risk Management. 2005
ICH Harmonised Tripartite Guideline. Q10-Pharmaceutical Quality System. 2008
Bill S. The inventors of six sigma. 2005
Juran JM. Juran on Quality by Design: The new steps for planning quality into goods and services. Free Press, New York: USA. 1992
Juran Trilogy: Quality assurance. 2007 Available on line: https://blogs.mtu.edu/ improvement/2014/02/27/the-juran-trilogy/
Singh B. QbD in Pharma product development life cycle. Chron Pharmabiz. 2013; 28: 72-79
Singh B, Beg S, Sharma G, Jain A, Negi P. Holistic application of Quality by Design (QbD) for pharma product development excellence and regulatory compliance. Nirma University J Pharm Sci. 2014; 1 (1): 19-35
Singh B, Raza K, Beg S. Developing “Optimized” drug products employing “Designed” experiments. Chem Ind Digest. 2013; June: 70-76
Lionberger RA, Lee SL, Lee L, Raw A, Yu LX. Quality by design: concepts for ANDAs. AAPS J. 2008; 10: 268-76
Yu LX, Amidon G, Khan MA, Hoag SW, Polli J, Raju GK, Woodcock, J. Understanding pharmaceutical Quality by Design. AAPS J. 2014; 16 (4): 771–783
Singh B. Quality by Design (QbD) for holistic pharma excellence and regulatory compliance. The Pharma Times. 2014; 46 (8): 26-33
Drakulich A. An enhanced approach to drug-substance development and manufacture. Pharm Tech. 2012; 36 (2): 1-4
Arnum PA. Quality by Design in excipients. Pharm Tech. 2013; 37 (2): 1-3
ICH Harmonised Tripartite Guideline. Q11-Development and Manufacture of Drug Substances. 2012
Bhutani H, Kurmi M, Singh S, Beg S, Singh B. Quality by Design (QbD) in analytical sciences: An overview. The Pharma Times. 2014; 46 (8): 71-75
Reid GL, Morgado J, Barnett K, Harrington B, Wang J, Harwood J, Fortin D. Analytical Quality by design (AQbD) in pharmaceutical development. Amr Pharma Rev. 2013, Available online at: www.americanpharmaceuticalreview.com
Dickinson PA, Lee WW, Stott PW, Townsend AI, Smart JP, Ghahramani P, Hammett T, Billett L, Behn S, Gibb RC, Abrahamsson B. Clinical relevance of dissolution testing in Quality by Design. AAPS J. 2008; 10 (2): 380–390
Chatterjee S. QbD principles for packaging design and stability: A regulatory perspective. AICHE Annual Meeting. October 17, 2011. Available online at: http://www.cbinet.com/sites/default/ files/files/Krumenaker_QBD_SC%20AICHE%20Mtg%20101011_V2.pdf (Accessed on 17 November 2016)
Stier E. FDA recommendations for ANDAs based on QbD: A bioequivalence case study. 44ème Congrès International SFSTP. June 6-7, 2012. Available online at: http://congres.sfstp. myevent.evenium.com/uploads/event_member/85118/20ethanstier.pdf
Sprenger K, Nickerson D, O’Connell AM, Morrison BW. Quality by Design in clinical trials: A collaborative pilot with FDA. Ther Innov Reg Sci. 2012
This website uses cookies to enable, optimise and analyse site operations, as well as to provide personalised content and allow you to connect to social media. By clicking "I agree" you consent to the use of cookies for non-essential functions and the related processing of personal data. You can adjust your cookie and associated data processing preferences at any time via our "Cookie Settings". Please view our Cookie Policy to learn more about the use of cookies on our website.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorised as ”Necessary” are stored on your browser as they are as essential for the working of basic functionalities of the website. For our other types of cookies “Advertising & Targeting”, “Analytics” and “Performance”, these help us analyse and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these different types of cookies. But opting out of some of these cookies may have an effect on your browsing experience. You can adjust the available sliders to ‘Enabled’ or ‘Disabled’, then click ‘Save and Accept’. View our Cookie Policy page.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Cookie
Description
cookielawinfo-checkbox-advertising-targeting
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertising & Targeting".
cookielawinfo-checkbox-analytics
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Analytics".
cookielawinfo-checkbox-necessary
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Performance".
PHPSESSID
This cookie is native to PHP applications. The cookie is used to store and identify a users' unique session ID for the purpose of managing user session on the website. The cookie is a session cookies and is deleted when all the browser windows are closed.
viewed_cookie_policy
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
zmember_logged
This session cookie is served by our membership/subscription system and controls whether you are able to see content which is only available to logged in users.
Performance cookies are includes cookies that deliver enhanced functionalities of the website, such as caching. These cookies do not store any personal information.
Cookie
Description
cf_ob_info
This cookie is set by Cloudflare content delivery network and, in conjunction with the cookie 'cf_use_ob', is used to determine whether it should continue serving “Always Online” until the cookie expires.
cf_use_ob
This cookie is set by Cloudflare content delivery network and is used to determine whether it should continue serving “Always Online” until the cookie expires.
free_subscription_only
This session cookie is served by our membership/subscription system and controls which types of content you are able to access.
ls_smartpush
This cookie is set by Litespeed Server and allows the server to store settings to help improve performance of the site.
one_signal_sdk_db
This cookie is set by OneSignal push notifications and is used for storing user preferences in connection with their notification permission status.
YSC
This cookie is set by Youtube and is used to track the views of embedded videos.
Analytics cookies collect information about your use of the content, and in combination with previously collected information, are used to measure, understand, and report on your usage of this website.
Cookie
Description
bcookie
This cookie is set by LinkedIn. The purpose of the cookie is to enable LinkedIn functionalities on the page.
GPS
This cookie is set by YouTube and registers a unique ID for tracking users based on their geographical location
lang
This cookie is set by LinkedIn and is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
lidc
This cookie is set by LinkedIn and used for routing.
lissc
This cookie is set by LinkedIn share Buttons and ad tags.
vuid
We embed videos from our official Vimeo channel. When you press play, Vimeo will drop third party cookies to enable the video to play and to see how long a viewer has watched the video. This cookie does not track individuals.
wow.anonymousId
This cookie is set by Spotler and tracks an anonymous visitor ID.
wow.schedule
This cookie is set by Spotler and enables it to track the Load Balance Session Queue.
wow.session
This cookie is set by Spotler to track the Internet Information Services (IIS) session state.
wow.utmvalues
This cookie is set by Spotler and stores the UTM values for the session. UTM values are specific text strings that are appended to URLs that allow Communigator to track the URLs and the UTM values when they get clicked on.
_ga
This cookie is set by Google Analytics and is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. It stores information anonymously and assign a randomly generated number to identify unique visitors.
_gat
This cookies is set by Google Universal Analytics to throttle the request rate to limit the collection of data on high traffic sites.
_gid
This cookie is set by Google Analytics and is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visited in an anonymous form.
Advertising and targeting cookies help us provide our visitors with relevant ads and marketing campaigns.
Cookie
Description
advanced_ads_browser_width
This cookie is set by Advanced Ads and measures the browser width.
advanced_ads_page_impressions
This cookie is set by Advanced Ads and measures the number of previous page impressions.
advanced_ads_pro_server_info
This cookie is set by Advanced Ads and sets geo-location, user role and user capabilities. It is used by cache busting in Advanced Ads Pro when the appropriate visitor conditions are used.
advanced_ads_pro_visitor_referrer
This cookie is set by Advanced Ads and sets the referrer URL.
bscookie
This cookie is a browser ID cookie set by LinkedIn share Buttons and ad tags.
IDE
This cookie is set by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
li_sugr
This cookie is set by LinkedIn and is used for tracking.
UserMatchHistory
This cookie is set by Linkedin and is used to track visitors on multiple websites, in order to present relevant advertisement based on the visitor's preferences.
VISITOR_INFO1_LIVE
This cookie is set by YouTube. Used to track the information of the embedded YouTube videos on a website.




 SARWAR BEG, PhD is a Research Scientist at Jubilant Generics Limited, Noida, India. His major areas of research interest include QbD-driven development and characterisation of diverse drug delivery systems. To date he has authored more than 90 research/review publications in several peer-reviewed journals, 15 book chapters, four books, three Indian patent applications with h-index of 16 and several young scientist awards to his credit. Moreover, he is serving as the Regional Editor of Current Nanomedicine, Editorial Board Member of Bioavailability and Bioequivalence Journal and Nanotech Research Letter, and reviewer of several international journals.
SARWAR BEG, PhD is a Research Scientist at Jubilant Generics Limited, Noida, India. His major areas of research interest include QbD-driven development and characterisation of diverse drug delivery systems. To date he has authored more than 90 research/review publications in several peer-reviewed journals, 15 book chapters, four books, three Indian patent applications with h-index of 16 and several young scientist awards to his credit. Moreover, he is serving as the Regional Editor of Current Nanomedicine, Editorial Board Member of Bioavailability and Bioequivalence Journal and Nanotech Research Letter, and reviewer of several international journals. MAHFOOZUR RAHMAN is an Assistant Professor at the Department of Pharmaceutical Sciences, Faculty of Health Sciences, Sam Higginbottom Institute of Agriculture, Technology & Sciences (SHIATS), Allahabad, India. He completed his Masters in Pharmacy in 2010 from Jamia Hamdard, New Delhi, India. His major areas of research interest include development and characterisation of nano-size drug delivery systems for inflammatory disorders. To date he has published over 50 publications in peer reviewed journals with H-index of 12 and eight book chapters with various reputed publishers. He is a member of IPGA and editorial board member of various journals.
MAHFOOZUR RAHMAN is an Assistant Professor at the Department of Pharmaceutical Sciences, Faculty of Health Sciences, Sam Higginbottom Institute of Agriculture, Technology & Sciences (SHIATS), Allahabad, India. He completed his Masters in Pharmacy in 2010 from Jamia Hamdard, New Delhi, India. His major areas of research interest include development and characterisation of nano-size drug delivery systems for inflammatory disorders. To date he has published over 50 publications in peer reviewed journals with H-index of 12 and eight book chapters with various reputed publishers. He is a member of IPGA and editorial board member of various journals. MR SAGAR SUMAN PANDA is currently working as an Assistant Professor at Roland Institute of Pharmaceutical Sciences, Berhampur, Odisha, India. Mr Panda has seven years of teaching experience in pharmaceutical analysis and major research interest in QbD-based analytical method development and validation. He has over 35 research publications in various peer-reviewed journals, one book on analytical QbD and several conference presentations to his credit.
MR SAGAR SUMAN PANDA is currently working as an Assistant Professor at Roland Institute of Pharmaceutical Sciences, Berhampur, Odisha, India. Mr Panda has seven years of teaching experience in pharmaceutical analysis and major research interest in QbD-based analytical method development and validation. He has over 35 research publications in various peer-reviewed journals, one book on analytical QbD and several conference presentations to his credit.




