Earlier this year, MGC Pharmaceuticals, in collaboration with the Slovenian National Institute of Biology (NIB) and the Neurosurgery Department at the University Medical Centre in Ljubljana, Slovenia, announced successful research results for their novel cannabinoid formulation, which has been developed for the treatment of glioblastoma. This article highlights the key study findings and their future research plans.
The goal of finding a “cure” for cancer has recently been replaced with the aim of taming tumour malignancy, turning cancer into a chronic disease with prolonged life expectancy and an improved quality of life. This strategy has been successful in some cancers; however, for glioblastoma, one of the most aggressive cancers, average survival has only increased by around 15 percent over the last 20 years.
This webinar showcases the Growth Direct System; an RMM (Rapid Microbial Method) that improves on traditional membrane filtration, delivering increased accuracy, a faster time to result, enhanced data integrity compliance, and more control over the manufacturing process.
Key learning points:
Understand the benefits of full workflow microbiology quality control testing automation in radiopharmaceutical production
Learn about ITM’s implementation journey and considerations when evaluating the technology
Find out how the advanced optics and microcolony detection capabilities of Growth Direct® technology impact time to result (TTR).
Don’t miss your chance to learn from experts in the industry –Register for FREE
Can’t attend live? No worries – register to receive the recording post-event.
Glioblastoma remains one of the most malignant cancer types despite the modern modalities of chemotherapy and irradiation treatment. Several phytochemicals exhibit important properties against this form of cancer, including the cannabinoids delta-9-tetrahydrocannabinol (THC) and cannabidiol (CBD) from Cannabis sativa. These bind to specific transmembrane proteins which are highly expressed on the tumour cell surface and facilitate entrance into the glioblastoma cells. Once inside, the cannabinoids interfere with specific biochemical pathways, promote tumour cells’ growth arrest, inhibit their invasion and cause cell death. In over 20 animal studies, CBD/THC was found to drastically decrease the size of and even eliminate glioblastoma. Furthermore, in a few clinical trials and published reports, the variable anti-glioblastoma effects of these two cannabinoids, in combination with other therapeutic modalities, have been demonstrated. However, wider clinical application of these preparations is hindered due to the psychotropic effects of THC. This often limits the clinical usage of THC and CBD mixtures in glioblastoma patients as many will already present with adverse neuropsychiatric symptoms, including impaired cognition.
The aim of the MGC research teams from the NIB, in collaboration with the Neurosurgery Department at the University Medical Centre in Ljubljana, Slovenia, was to develop cannabinoid formulations and define protocols for the treatment of glioblastoma patients, focusing on glioblastoma stem cell (GSC) antagonists. These include the most effective cannabinoid combinations alone and with the standard therapeutic, temozolomide (TMZ). Specifically, their aim was to assess the influence of three natural cannabinoids – THC, CBD and cannabigerol (CBG) – on cell viability and apoptosis in vitro in three-dimensional (3D) spheroids and in vivo in experimental animals.
Addressing current challenges in glioblastoma therapy
The MGC research team established a postoperative, pre-treatment diagnostic platform, where the response of patients’ primary tumour cells to the most effective cannabinoid preparation was determined and correlated with the individual tumour cells’ genetics. This diagnostic platform is highly innovative as it addresses the three major reasons for inefficacy in current glioblastoma therapy.
The first obstacle is glioblastoma heterogeneity. The MGC scientists assumed that in vitro tumour cell responses may be different in each patient: 1) they would have one of four specific glioblastoma subtype tumours or 2) a unique pattern of at least five major cannabinoid cell surface receptors. If, and when, a correlation is observed using bioinformatic tools, such information would enable a patient-tailored cannabinoid formulation to be applied in his/her treatment, administered at an early stage. This may be relevant when translated to Phase I clinical trials.
This diagnostic platform is highly innovative as it addresses the three major reasons for inefficacy in current glioblastoma therapy”
Secondly, it is generally not known if and how patients’ GSCs are affected by various cannabinoids. This sub-population of cancer cells, which evolve during cancer progression by acquiring intrinsic resistance to irradiation, is at present considered the key therapeutic target. We, and others, have demonstrated CBD cytotoxic killing of GSCs whereby CBD induces an increase in damaging free radicals and others that led to the inhibition of GSCs dedifferentiation, death in vivo and even prolonged the survival of tumour-bearing mice by CBD.
THC also affects glioblastoma cell death through CB1 receptor-mediated signalling, acting in synergy with CBD. However, the third obstacle preventing cannabinoid translation from lab bench to patient’s bed is THC’s psychoactive effect, which may counteract the palliative cannabinoid benefits in glioblastoma patients, who may be losing their cognitive perceptions and stability due to disease progression.
Study findings
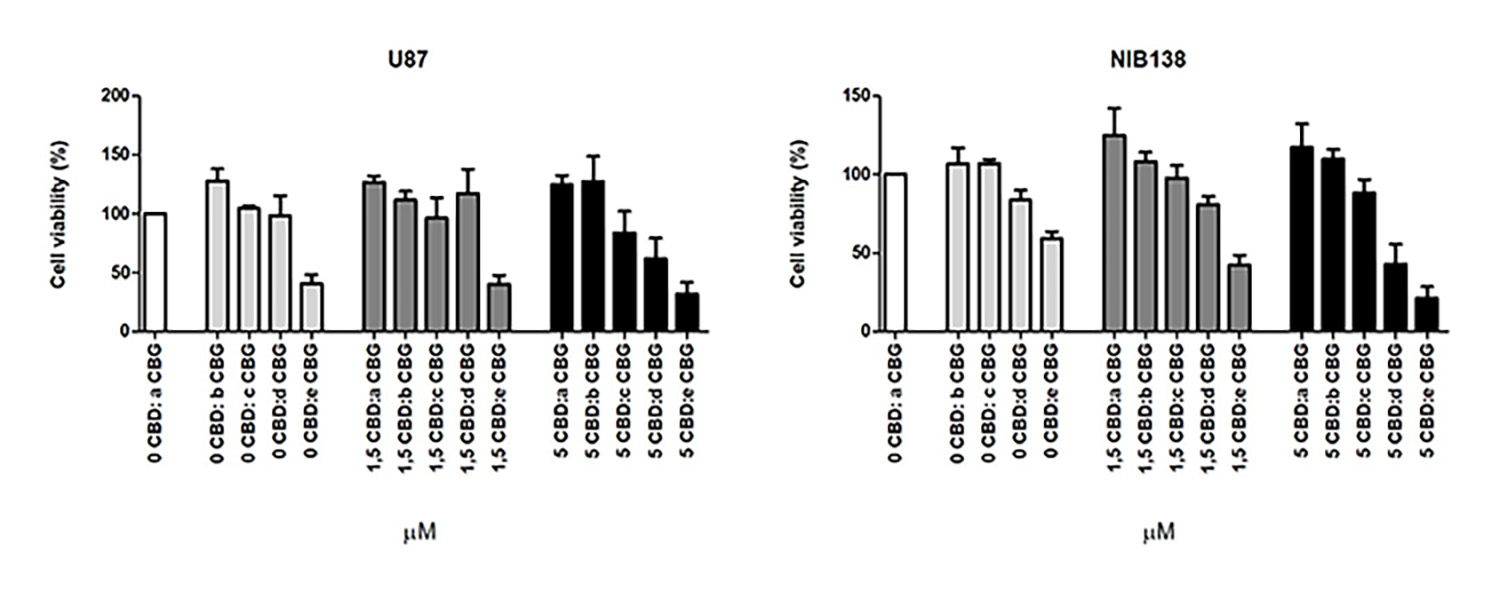
The present study investigated CBG, an additional non-intoxicating cannabinoid with little known about its potential as an anti-cancer agent. We found that adding CBG to CBD can double the cytotoxic effect on glioblastoma cells. While CBD inhibits the glioblastoma cells’ viability, CBG appears to be more efficient at inducing the cascade of biological processes leading to programmed death (apoptosis) of GSCs (Figure 1).
Figure 1: Shows cell viability inhibition of model GB cell line U87 and NIB138 GB cells after CBDM and CBGM combination treatments.
The effective power of CBG and CBD to terminate cancer stem cells is completely novel. The ability of this formulation to affect GSCs in vivo, without the need for THC, would enable the development of a therapeutic intervention which is devoid of its psychotropic effects.
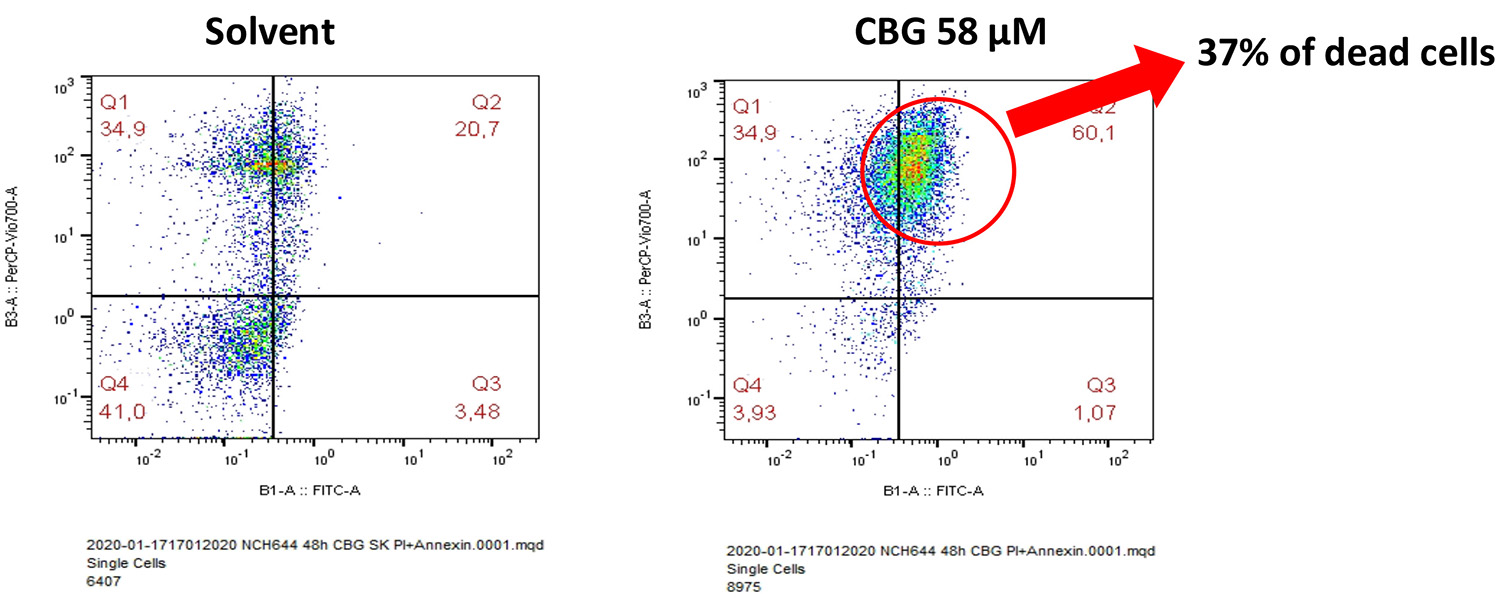
Figure 2 shows our results that demonstrate CBG also affects the survival of GSCs. This observation is significant as these cells tend to survive the initial treatment and multiply, leading to tumour recurrence. Although these cell lines are extremely resistant to irradiation and chemotherapy, they appear to be sensitive to CBG, as shown in our experiments, where we demonstrated the death of one third of the cells exposed to a milieu with a concentration of circa 50μM of CBG.
Figure 2: A solvent control, comprised of solvent dimethyl sulfoxide and ethanol, was compared to each of the mono ingredients. Right: NCH644 cells – glioblastoma stem cell line 48 hours after addition of 58μMol of CBG. Thirty-seven percent of the cells were dead.
Next steps
Our research is now focused on testing delivery systems, with the aim to cross the blood-brain barrier (BBB). This will be tested in a suitable zebra fish embryo model, established for glioblastoma research at NIB. Due to leaky tumour vasculature, it is expected that drug diffusion to highly angiogenic glioblastoma mass will be much easier than that seen in neurodegenerative diseases.
Novel formulations of nanomaterials for cannabinoid encapsulation, mostly comprising CBD and CBG, are being tested to target patient-derived GSCs in 3D spheroid cultures in vitro. The tumorous raised from engrafted patient-derived GSCs will then be exposed to encapsulated cannabinoids and, due to the animal transparency, glioblastoma growth and invasion in the fish brain will be easy to analyse, while fluorescently tagged GSCs may reveal the mechanism of cannabinoid activity in the brain tumour.
The team believes this research may have wider implications for the use of cannabinoid compounds in the treatment of the brain tumours and possibly brain metastases. It is hoped that these results will aid our understanding of precision treatment design regimens for potential formulations of adjuvant therapies. These would be designed and followed in a Phase I/II clinical study of cannabinoids, focusing on the novel effects of CBG in glioblastoma patients. As cannabinoids are already used by oncologists for palliative effects, we hope to propose the early and informative postoperative use of cannabinoids in glioblastoma that would also fully exploit their assumed anti-tumour activity.
Conclusions
The aim of the present research was to use specific cannabinoids to develop in vitro formulations and define the protocols for the treatment of glioblastoma alone in the first phase of treatment, rather than as a “second or last choice”. We believe, based on current knowledge, that combinatorial therapy is needed in all cancers and that cannabinoids will serve to be an add-on therapeutic, with the main advantage to lower doses of harmful chemotherapy and irradiation.
No significant side effects of CBD have been observed in glioblastoma patients, however unpredictable THC effects should be avoided. Our study is the first to open the possibility of replacing THC with CBG, which is highly effective in killing GSCs – the “root” of the tumour growth. The question of specific ratios, customised to patient tumour genetics, will be addressed after a statistically relevant number of glioblastoma patients have been included in this study. To conclude, targeting GSCs with these cannabinoids may significantly improve standard disease treatment for glioblastoma.
About the author
Professor Tamara Lah holds a PhD from the University of Ljubljana, Slovenia and is the former Director of the National Institute of Biology and established Department of Genetic Toxicology and Cancer Biology. At present, she is a Scientific Councillor and professor of Cancer Biology at the University of Ljubljana. She has previously worked at Josef Stefan Institute in Slovenia and the University of Newcastle upon Tyne, UK. She also was a postdoc and Assistant Professor at the School of Medicine in WSU in Detroit, Director of Metastasis Research Laboratory at Albert Einstein Medical Centre, in Philadelphia, PA and recently a Visiting Professor in Sao Paolo University in Brasil.
This website uses cookies to enable, optimise and analyse site operations, as well as to provide personalised content and allow you to connect to social media. By clicking "I agree" you consent to the use of cookies for non-essential functions and the related processing of personal data. You can adjust your cookie and associated data processing preferences at any time via our "Cookie Settings". Please view our Cookie Policy to learn more about the use of cookies on our website.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorised as ”Necessary” are stored on your browser as they are as essential for the working of basic functionalities of the website. For our other types of cookies “Advertising & Targeting”, “Analytics” and “Performance”, these help us analyse and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these different types of cookies. But opting out of some of these cookies may have an effect on your browsing experience. You can adjust the available sliders to ‘Enabled’ or ‘Disabled’, then click ‘Save and Accept’. View our Cookie Policy page.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Cookie
Description
cookielawinfo-checkbox-advertising-targeting
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertising & Targeting".
cookielawinfo-checkbox-analytics
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Analytics".
cookielawinfo-checkbox-necessary
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Performance".
PHPSESSID
This cookie is native to PHP applications. The cookie is used to store and identify a users' unique session ID for the purpose of managing user session on the website. The cookie is a session cookies and is deleted when all the browser windows are closed.
viewed_cookie_policy
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
zmember_logged
This session cookie is served by our membership/subscription system and controls whether you are able to see content which is only available to logged in users.
Performance cookies are includes cookies that deliver enhanced functionalities of the website, such as caching. These cookies do not store any personal information.
Cookie
Description
cf_ob_info
This cookie is set by Cloudflare content delivery network and, in conjunction with the cookie 'cf_use_ob', is used to determine whether it should continue serving “Always Online” until the cookie expires.
cf_use_ob
This cookie is set by Cloudflare content delivery network and is used to determine whether it should continue serving “Always Online” until the cookie expires.
free_subscription_only
This session cookie is served by our membership/subscription system and controls which types of content you are able to access.
ls_smartpush
This cookie is set by Litespeed Server and allows the server to store settings to help improve performance of the site.
one_signal_sdk_db
This cookie is set by OneSignal push notifications and is used for storing user preferences in connection with their notification permission status.
YSC
This cookie is set by Youtube and is used to track the views of embedded videos.
Analytics cookies collect information about your use of the content, and in combination with previously collected information, are used to measure, understand, and report on your usage of this website.
Cookie
Description
bcookie
This cookie is set by LinkedIn. The purpose of the cookie is to enable LinkedIn functionalities on the page.
GPS
This cookie is set by YouTube and registers a unique ID for tracking users based on their geographical location
lang
This cookie is set by LinkedIn and is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
lidc
This cookie is set by LinkedIn and used for routing.
lissc
This cookie is set by LinkedIn share Buttons and ad tags.
vuid
We embed videos from our official Vimeo channel. When you press play, Vimeo will drop third party cookies to enable the video to play and to see how long a viewer has watched the video. This cookie does not track individuals.
wow.anonymousId
This cookie is set by Spotler and tracks an anonymous visitor ID.
wow.schedule
This cookie is set by Spotler and enables it to track the Load Balance Session Queue.
wow.session
This cookie is set by Spotler to track the Internet Information Services (IIS) session state.
wow.utmvalues
This cookie is set by Spotler and stores the UTM values for the session. UTM values are specific text strings that are appended to URLs that allow Communigator to track the URLs and the UTM values when they get clicked on.
_ga
This cookie is set by Google Analytics and is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. It stores information anonymously and assign a randomly generated number to identify unique visitors.
_gat
This cookies is set by Google Universal Analytics to throttle the request rate to limit the collection of data on high traffic sites.
_gid
This cookie is set by Google Analytics and is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visited in an anonymous form.
Advertising and targeting cookies help us provide our visitors with relevant ads and marketing campaigns.
Cookie
Description
advanced_ads_browser_width
This cookie is set by Advanced Ads and measures the browser width.
advanced_ads_page_impressions
This cookie is set by Advanced Ads and measures the number of previous page impressions.
advanced_ads_pro_server_info
This cookie is set by Advanced Ads and sets geo-location, user role and user capabilities. It is used by cache busting in Advanced Ads Pro when the appropriate visitor conditions are used.
advanced_ads_pro_visitor_referrer
This cookie is set by Advanced Ads and sets the referrer URL.
bscookie
This cookie is a browser ID cookie set by LinkedIn share Buttons and ad tags.
IDE
This cookie is set by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
li_sugr
This cookie is set by LinkedIn and is used for tracking.
UserMatchHistory
This cookie is set by Linkedin and is used to track visitors on multiple websites, in order to present relevant advertisement based on the visitor's preferences.
VISITOR_INFO1_LIVE
This cookie is set by YouTube. Used to track the information of the embedded YouTube videos on a website.