Dr Martin Goldman joins Peter Brady, Orbital Media’s CEO, to discuss how to untap the potential of social media sourced real world evidence…
Whilst newspapers make much of clinical trials that go wrong and patients come to harm, they never mention the ones that go wrong and don’t harm patients. A common scenario for this failing is simply being unable to recruit the planned number of patients either because of overoptimistic estimates of recruitment or studies that are just plain overcomplicated.
This webinar showcases the Growth Direct System; an RMM (Rapid Microbial Method) that improves on traditional membrane filtration, delivering increased accuracy, a faster time to result, enhanced data integrity compliance, and more control over the manufacturing process.
Key learning points:
Understand the benefits of full workflow microbiology quality control testing automation in radiopharmaceutical production
Learn about ITM’s implementation journey and considerations when evaluating the technology
Find out how the advanced optics and microcolony detection capabilities of Growth Direct® technology impact time to result (TTR).
Don’t miss your chance to learn from experts in the industry –Register for FREE
A recent report on the Salford Lung Study indicated that for prospective randomised studies, the proportion of possible patients with asthma and COPD who meet the common inclusion criteria in randomised studies has been estimated to be as low as 3% and 7% respectively. It’s these figures that make you realise there has to be another way.
That alternative is real world evidence, and it has the potential to be an important part of the jigsaw of evidence, supporting new and old products. The name says it all, and real world studies tell you what is the evidence from real patients in the real world. It is an eye-opener for researchers to realise that there is a path to data and that the studies can have true meaning.
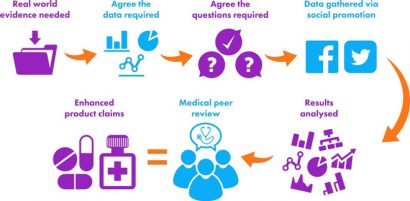
To generate real world evidence, there are three possible avenues.
Classic clinical study
There’s the classic clinical study, with a planned intervention but with an inbuilt patient experience reporting documenting their ‘real world’ e.g. patient reported outcome, but the population is limited by the trial inclusions and exclusion.
Hybrid study
The second is a hybrid study using existing databases to inform an overall study objective and support other research objectives by coupling the use of existing electronic record management data with prospective data collection from physicians and/or patients and caregivers. This approach was used in the Salford Lung Study to create a so-called pragmatic randomised clinical trial.
Retrospective collection of data
The third way is the retrospective collection of data. This typically has used existing data records such as large scale patient data (e.g. GPRD, yellow card). The problem with the first two is that by selecting patients for a prospective study, by definition the selected population may not be real.
History of real world evidence
Here is a historical example. Terodiline, an antimuscarinic and calcium antagonist drug, was used to treat detrusor instability but was withdrawn in 1991 after provoking serious ventricular arrhythmias associated with increases in the corrected QT interval (QTc).
The drug had been on the market for some time before this was recognised, and it did not manifest in the studies undertaken for drug authorisation and in early clinical use. An intense scientific review of ten patients published in an international medical journal was the signal.
However, a subsequent retrospective trawl through the real world data from the Green Card prescription event monitoring revealed an excess of reports of fits faints and funny turns compared to a control group. This was the real world evidence.
Now there are better ways to collect patient experiences, and recently attention has been turned to using social media. Once again, there is more than one potential approach to using this novel platform. One way is to engage with individuals prospectively who are in a normal healthcare environment or in a study and get them to feed back their experiences using a social media platform or smartphone application.
“[Patients can easily] feedback their experiences using a social media platform or smartphone application…”
However, this is an intervention of sorts and demands a discipline of regular involvement. Possible contexts for these would be real time management of asthma or diabetes based on symptoms and self-monitoring, and then feeding the data back into the electronic medical records.
This is sailing towards uncharted waters, and there are monsters out there that need to be tamed such as the ownership of data, if middlemen are involved, and data-protection issues, particularly if the data are not primarily part of the patients’ normal medical records.
Collecting large scale real world data
The use of social media platforms for retrospective collection of patient experience is a rapid inexpensive method for the collection of large-scale real world data. We have been running studies using social media to recruit patients and then involving them in tailor-made interactive self-administered evaluations.
“…4000 participants in 9 days…”
Because social media is so pervasive, the willingness of patients with common conditions to engage is gratifyingly large, and our best result was recruiting 4000 participants in 9 days. These types of studies are more classic RWE studies, with no exclusions (bar those absolutely necessary to determine if the patient is relevant), no restrictions on other medicines taken, and accepting the real life situation that the product under investigation may or may not be taken according to the instructions.
“…in its infancy but results so far have been gratifyingly encouraging…”
These are true intent to treat studies, and again, these do not examine compliance or how long the treatment has been used. This is the real world. So far we have only done open non-comparative studies as the complex problems of organising comparator groups, matching patients and engaging in some of the daunting statistical methods has not been solved.
Disadvantages of social media platforms
There are some weaknesses to this approach. The data by definition are open and retrospective. The evaluations of necessity are based on pragmatic experience, and this has entailed the use of some invalid measures, but this has not detracted from the usefulness of data. Another point is you cannot collect what the patients don’t know or have not experienced.
Whilst pilot studies have given clues as to the practicality, the final recruited numbers may sometimes only be guessed at. Setting a minimum number has been a useful step, and this has typically been based on what would be thought credible by the critical audience. Big numbers are possible and these add to the credibility as adjunct data to clinical trials.
The use of social media for collection of real world healthcare data is in its infancy but results so far have been gratifyingly encouraging.
Dr Martin Goldman trained as a gastroenterologist and is now a consulting pharmaceutical physician. After many years advising on the development and marketing of medicines, with the support of some very bright colleagues, he pioneered the concept of a novel methodology for conducting real-world evidence studies of healthcare using social media.
Peter Brady is Chief Executive Officer at Orbital Media, specialist social and digital agency. Having co-founded the company 13 years ago, he has specialised in working with consumer healthcare brands on digital and social innovation. Working in partnership with Dr Martin Goldman and other industry figures, Peter has spear-headed the development and implementation of a unique real-world evidence solution using social media.
This website uses cookies to enable, optimise and analyse site operations, as well as to provide personalised content and allow you to connect to social media. By clicking "I agree" you consent to the use of cookies for non-essential functions and the related processing of personal data. You can adjust your cookie and associated data processing preferences at any time via our "Cookie Settings". Please view our Cookie Policy to learn more about the use of cookies on our website.
This website uses cookies to improve your experience while you navigate through the website. Out of these cookies, the cookies that are categorised as ”Necessary” are stored on your browser as they are as essential for the working of basic functionalities of the website. For our other types of cookies “Advertising & Targeting”, “Analytics” and “Performance”, these help us analyse and understand how you use this website. These cookies will be stored in your browser only with your consent. You also have the option to opt-out of these different types of cookies. But opting out of some of these cookies may have an effect on your browsing experience. You can adjust the available sliders to ‘Enabled’ or ‘Disabled’, then click ‘Save and Accept’. View our Cookie Policy page.
Necessary cookies are absolutely essential for the website to function properly. This category only includes cookies that ensures basic functionalities and security features of the website. These cookies do not store any personal information.
Cookie
Description
cookielawinfo-checkbox-advertising-targeting
The cookie is set by GDPR cookie consent to record the user consent for the cookies in the category "Advertising & Targeting".
cookielawinfo-checkbox-analytics
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Analytics".
cookielawinfo-checkbox-necessary
This cookie is set by GDPR Cookie Consent plugin. The cookie is used to store the user consent for the cookies in the category "Necessary".
cookielawinfo-checkbox-performance
This cookie is set by GDPR Cookie Consent WordPress Plugin. The cookie is used to remember the user consent for the cookies under the category "Performance".
PHPSESSID
This cookie is native to PHP applications. The cookie is used to store and identify a users' unique session ID for the purpose of managing user session on the website. The cookie is a session cookies and is deleted when all the browser windows are closed.
viewed_cookie_policy
The cookie is set by the GDPR Cookie Consent plugin and is used to store whether or not user has consented to the use of cookies. It does not store any personal data.
zmember_logged
This session cookie is served by our membership/subscription system and controls whether you are able to see content which is only available to logged in users.
Performance cookies are includes cookies that deliver enhanced functionalities of the website, such as caching. These cookies do not store any personal information.
Cookie
Description
cf_ob_info
This cookie is set by Cloudflare content delivery network and, in conjunction with the cookie 'cf_use_ob', is used to determine whether it should continue serving “Always Online” until the cookie expires.
cf_use_ob
This cookie is set by Cloudflare content delivery network and is used to determine whether it should continue serving “Always Online” until the cookie expires.
free_subscription_only
This session cookie is served by our membership/subscription system and controls which types of content you are able to access.
ls_smartpush
This cookie is set by Litespeed Server and allows the server to store settings to help improve performance of the site.
one_signal_sdk_db
This cookie is set by OneSignal push notifications and is used for storing user preferences in connection with their notification permission status.
YSC
This cookie is set by Youtube and is used to track the views of embedded videos.
Analytics cookies collect information about your use of the content, and in combination with previously collected information, are used to measure, understand, and report on your usage of this website.
Cookie
Description
bcookie
This cookie is set by LinkedIn. The purpose of the cookie is to enable LinkedIn functionalities on the page.
GPS
This cookie is set by YouTube and registers a unique ID for tracking users based on their geographical location
lang
This cookie is set by LinkedIn and is used to store the language preferences of a user to serve up content in that stored language the next time user visit the website.
lidc
This cookie is set by LinkedIn and used for routing.
lissc
This cookie is set by LinkedIn share Buttons and ad tags.
vuid
We embed videos from our official Vimeo channel. When you press play, Vimeo will drop third party cookies to enable the video to play and to see how long a viewer has watched the video. This cookie does not track individuals.
wow.anonymousId
This cookie is set by Spotler and tracks an anonymous visitor ID.
wow.schedule
This cookie is set by Spotler and enables it to track the Load Balance Session Queue.
wow.session
This cookie is set by Spotler to track the Internet Information Services (IIS) session state.
wow.utmvalues
This cookie is set by Spotler and stores the UTM values for the session. UTM values are specific text strings that are appended to URLs that allow Communigator to track the URLs and the UTM values when they get clicked on.
_ga
This cookie is set by Google Analytics and is used to calculate visitor, session, campaign data and keep track of site usage for the site's analytics report. It stores information anonymously and assign a randomly generated number to identify unique visitors.
_gat
This cookies is set by Google Universal Analytics to throttle the request rate to limit the collection of data on high traffic sites.
_gid
This cookie is set by Google Analytics and is used to store information of how visitors use a website and helps in creating an analytics report of how the website is doing. The data collected including the number visitors, the source where they have come from, and the pages visited in an anonymous form.
Advertising and targeting cookies help us provide our visitors with relevant ads and marketing campaigns.
Cookie
Description
advanced_ads_browser_width
This cookie is set by Advanced Ads and measures the browser width.
advanced_ads_page_impressions
This cookie is set by Advanced Ads and measures the number of previous page impressions.
advanced_ads_pro_server_info
This cookie is set by Advanced Ads and sets geo-location, user role and user capabilities. It is used by cache busting in Advanced Ads Pro when the appropriate visitor conditions are used.
advanced_ads_pro_visitor_referrer
This cookie is set by Advanced Ads and sets the referrer URL.
bscookie
This cookie is a browser ID cookie set by LinkedIn share Buttons and ad tags.
IDE
This cookie is set by Google DoubleClick and stores information about how the user uses the website and any other advertisement before visiting the website. This is used to present users with ads that are relevant to them according to the user profile.
li_sugr
This cookie is set by LinkedIn and is used for tracking.
UserMatchHistory
This cookie is set by Linkedin and is used to track visitors on multiple websites, in order to present relevant advertisement based on the visitor's preferences.
VISITOR_INFO1_LIVE
This cookie is set by YouTube. Used to track the information of the embedded YouTube videos on a website.